
Abdominal Assessment for Student Paramedics: A Practical Guide to Assessing Abdominal Pain
Part 1 - Introduction
Abdominal pain is one of the most common reasons people call an ambulance, yet it remains one of the most challenging presentations for student paramedics to assess confidently.
Unlike chest pain or major trauma, abdominal pain rarely follows a predictable pattern. Two patients with the same underlying condition can present completely differently. A patient with mild discomfort may be harbouring life-threatening pathology, while another with severe pain may have a condition that can safely be managed without emergency intervention.
This uncertainty is what makes abdominal assessment difficult.
For many students, the challenge is not remembering what questions to ask. It is understanding why those questions matter and how the answers influence your clinical decision-making.
Your role as a paramedic is not to make a definitive diagnosis at the roadside. Without blood tests, CT imaging or ultrasound, that would often be impossible. Instead, your responsibility is to:
Recognise patients who are critically unwell
Identify red flags that suggest serious pathology
Gather enough information to form a safe working impression
Begin appropriate treatment where indicated
Decide whether the patient requires immediate hospital assessment
Clearly communicate and document your findings
Every part of your assessment should move you closer to answering one simple question:
"How worried should I be about this patient?"
That question should remain in your mind from the moment you arrive until the patient is safely handed over.
Why abdominal pain is so difficult to assess
One of the biggest misconceptions among student paramedics is believing there is a simple algorithm that tells you exactly what condition a patient has.
Unfortunately, abdominal pain doesn't work like that.
Many abdominal conditions share remarkably similar symptoms.
For example:
Appendicitis may initially present with vague central abdominal pain before localising to the right iliac fossa.
An abdominal aortic aneurysm may present as back pain.
Myocardial infarction can present solely with epigastric discomfort.
Lower lobe pneumonia may cause upper abdominal pain.
Diabetic ketoacidosis commonly presents with abdominal pain and vomiting.
Ectopic pregnancy may initially appear to be simple abdominal discomfort.
This is why experienced clinicians rarely ask:
"What is the diagnosis?"
Instead they ask:
"What serious conditions do I need to consider, and how can I safely narrow my differential diagnosis?"
That subtle shift in thinking is what separates checklist assessment from clinical reasoning.
Clinical Pearl
Patients don't read textbooks.
Many serious abdominal conditions present atypically.
Never dismiss a patient simply because they don't fit the "classic" presentation you learnt at university.
Understanding the abdomen (without making anatomy painful)
Before assessing abdominal pain, it helps to understand why clinicians divide the abdomen into different regions.
Patients often struggle to accurately describe where pain originates.
One patient may describe "stomach pain" while pointing to the epigastrium.
Another may simply point to the whole abdomen.
Breaking the abdomen into regions allows clinicians to relate symptoms to the organs most likely to be involved.
Although pathology is never completely predictable, regional pain immediately begins to shape your differential diagnosis.
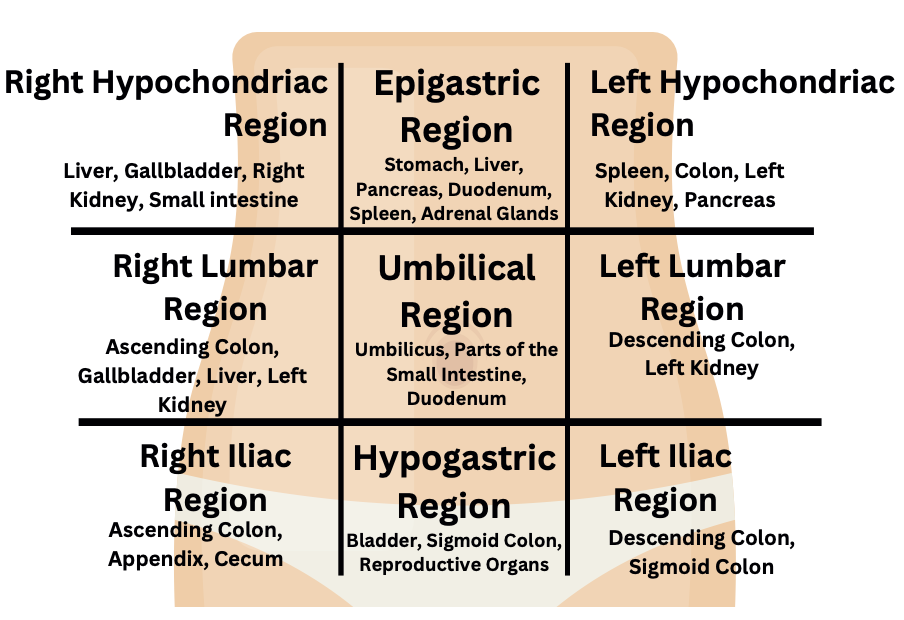
The Nine Regions
Make it stand out
The abdomen is split into 9 regions. The right and left hypochondriac regions and epigastric region at the top.
The right and left lumbar regions and umbilical region in the middle.
And right and left iliac regions and hypogastric region at the bottom.
Right hypochondrium
Contains structures including:
Liver
Gallbladder
Hepatic flexure
Upper pole of the right kidney
Pain here may suggest:
Cholecystitis
Biliary colic
Hepatitis
Liver pathology
Epigastrium
Contains:
Stomach
Pancreas
Duodenum
Part of the liver
Pain here may be associated with:
Gastritis
Peptic ulcer disease
Pancreatitis
Early myocardial infarction
Notice that one of those conditions isn't actually abdominal in origin.
This is why abdominal pain should never be assessed in isolation from the rest of the patient.
Left hypochondrium
Contains:
Spleen
Stomach
Tail of the pancreas
Upper left kidney
Potential pathology includes:
Splenic injury
Gastritis
Pancreatitis
Right lumbar region
Includes:
Ascending colon
Right kidney
Small bowel
Pain here may suggest:
Renal colic
Pyelonephritis
Colitis
Umbilical region
Contains:
Small bowel
Part of the transverse colon
Major abdominal vessels
Many conditions begin with vague periumbilical pain before becoming more localised.
Appendicitis is the classic example.
Left lumbar region
Includes:
Descending colon
Left kidney
Common differentials include:
Diverticular disease
Renal pathology
Right iliac fossa
The area every student immediately associates with appendicitis.
Although appendicitis is important, don't forget:
Crohn's disease
Ovarian pathology
Ectopic pregnancy
Renal colic
Mesenteric adenitis
Suprapubic region
Contains:
Bladder
Uterus
Distal bowel
Pain may indicate:
Urinary retention
Urinary tract infection
Pelvic inflammatory disease
Pregnancy-related pathology
Left iliac fossa
Most commonly associated with:
Diverticulitis
Constipation
Ovarian pathology
Colitis
Think Like a Paramedic
Regional pain is only one piece of the puzzle.
Patients don't always present with pain exactly where the pathology is located.
Pain can:
Refer
Migrate
Become generalised
Be poorly localised
Never anchor your diagnosis solely on location.
Instead, use pain location as one clue among many.
Before you ask a single question
One of the biggest differences between experienced clinicians and students is that experienced clinicians begin assessing the patient before introductions are even complete.
Within seconds, they are subconsciously asking themselves:
Does this patient look ill?
Are they moving normally?
Are they pale?
Are they sweating?
Are they protecting their abdomen?
Are they lying completely still?
Are they restless and unable to get comfortable?
Are they speaking in full sentences?
These observations often provide more useful information than the first five minutes of questioning.
For example:
A patient with peritonitis often lies very still because movement worsens the pain.
Conversely, patients with renal colic are frequently unable to stay still, constantly changing position in an attempt to become comfortable.
These behavioural differences are not diagnostic, but they provide valuable clues that should influence your thinking from the very beginning.
Common Student Mistake
Many students become so focused on remembering their history-taking framework that they forget to observe the patient.
Before you ask your first question, spend a few seconds simply looking.
How is the patient sitting?
How are they breathing?
What does their face tell you?
Those observations are the beginning of your assessment, not an optional extra.
The Primary Survey Always Comes First
Regardless of the presenting complaint, every patient deserves a structured primary survey.
It can be tempting to jump straight into abdominal questioning when someone tells you they have stomach pain.
Resist that temptation.
Your first priority is to identify immediately life-threatening problems.
Ask yourself:
Is the airway patent?
Is the patient ventilating adequately?
Are they adequately perfused?
Is there evidence of shock?
Is there altered consciousness?
Remember:
Abdominal pain is a symptom, not a diagnosis.
Patients with abdominal pain can deteriorate because of:
Massive haemorrhage
Septic shock
Ruptured ectopic pregnancy
Abdominal aortic aneurysm
Bowel perforation
Identifying physiological instability early is far more important than immediately determining the exact cause of the pain.
PocketClinician Tip
One of the biggest challenges students face is remembering which questions to ask and which signs to look for when assessing abdominal pain.
The PocketClinician Student Paramedic Pocketbook includes a dedicated abdominal assessment section that takes you through:
A structured history-taking approach
Key abdominal examination findings
Important positive and negative signs
Red flags that should increase your suspicion of serious pathology
Documentation prompts to help you justify your clinical reasoning
It's designed to reduce cognitive overload on placement, allowing you to focus on the patient rather than trying to remember every step from memory.
Part 2 - History Taking: More Than Just SOCRATES
Every student paramedic learns a pain assessment framework such as SOCRATES or OPQRST.
These are excellent tools and should absolutely form part of your assessment.
However, they are not an abdominal assessment.
They are pain assessment tools.
Abdominal pain assessment extends far beyond the pain itself. Two patients may describe identical pain using SOCRATES, yet have completely different underlying pathology. Understanding the wider clinical picture is what separates a structured history from genuine clinical reasoning.
Throughout your history, keep asking yourself:
"How does this answer change my differential diagnosis?"
If the answer doesn't change your thinking, ask yourself whether the question was clinically useful.
Understanding the Pain
SOCRATES remains an excellent place to begin, but don't ask questions simply because they appear on a checklist.
Interpret every answer.
Site
Where is the pain?
Encourage the patient to point with one finger if possible.
Patients who sweep their entire hand across the abdomen often have poorly localised or diffuse pain, whereas localised pain can sometimes provide stronger diagnostic clues.
Remember that pain location may:
Migrate
Radiate
Become generalised
Refer to distant structures
Never assume the painful area is the diseased organ.
Onset
The onset of pain often provides one of the most valuable diagnostic clues.
Consider:
Sudden onset
Abdominal aortic aneurysm
Perforated viscus
Ovarian torsion
Testicular torsion
Renal colic
Gradual onset
Appendicitis
Diverticulitis
Cholecystitis
Gastroenteritis
Patients rarely remember exact times, but they often remember what they were doing when symptoms began.
Character
Patients frequently struggle to describe pain.
Avoid putting words into their mouth.
Instead ask:
"Can you describe what the pain feels like in your own words?"
Descriptions may include:
Sharp
Dull
Cramping
Burning
Colicky
Pressure-like
Colicky pain often reflects obstruction of a hollow organ, whereas constant pain may indicate inflammatory processes.
Again, these are clues—not diagnoses.
Radiation
Pain rarely stays where it begins.
Examples include:
Shoulder tip pain associated with diaphragmatic irritation
Back pain associated with pancreatitis or abdominal aortic aneurysm
Groin pain associated with renal colic
Understanding referred pain prevents clinicians from becoming anchored on one anatomical region.
Timing
Ask:
Has the pain been constant?
Does it come and go?
Has it changed since it began?
Pain that worsens steadily may suggest progressive inflammatory disease.
Pain that comes in waves often reflects obstruction or smooth muscle spasm.
Exacerbating and relieving factors
Simple questions often reveal useful clues.
Does movement make it worse?
Pain that increases significantly with movement may suggest peritoneal irritation.
Does eating affect the pain?
Pain after eating may suggest biliary disease.
Does leaning forwards help?
Some patients with pancreatitis find this position more comfortable.
Again, never interpret one answer in isolation.
Severity
Pain scores are useful—but only when interpreted alongside behaviour.
A patient reporting 10/10 pain while comfortably scrolling through their phone should not be dismissed, but it should encourage further assessment rather than blind acceptance.
Likewise, elderly patients frequently under-report pain despite serious pathology.
Pain scores should support assessment, not replace it.
Think Like a Paramedic
Patients are remarkably poor at diagnosing themselves.
Instead of asking:
"What do you think it is?"
Try asking:
"Tell me what has changed that made you decide to call today."
This often reveals the reason they became concerned and helps identify deterioration.
Looking Beyond the Pain
This is where abdominal assessment becomes far more powerful.
Students often spend ten minutes discussing pain characteristics while forgetting the symptoms that actually narrow the differential diagnosis.
Gastrointestinal symptoms
Nausea and vomiting
Ask:
When did it start?
Before or after the pain?
How many episodes?
What did it look like?
Vomiting before abdominal pain often points towards different pathology than vomiting after pain begins.
Consider whether the vomit contains:
Food
Bile
Fresh blood
Coffee-ground material
Fresh haematemesis is always concerning.
Coffee-ground vomit suggests older upper gastrointestinal bleeding.
Appetite
Loss of appetite is frequently overlooked.
Patients with appendicitis commonly report reduced appetite.
Although non-specific, it contributes to the overall clinical picture.
Bowel habit
Ask about:
Constipation
Diarrhoea
Last bowel movement
Ability to pass flatus
Failure to pass stool or wind may suggest bowel obstruction.
Diarrhoea may indicate:
Infection
Inflammatory bowel disease
Overflow from severe constipation
Again, interpretation depends on the wider history.
Blood in stool
Always clarify:
Fresh bright red blood?
Or black, tar-like stools?
Fresh bleeding often reflects lower gastrointestinal pathology.
Melena suggests upper gastrointestinal bleeding until proven otherwise.
Never assume patients know the difference.
Urinary Symptoms
Abdominal pain and urinary pathology frequently overlap.
Ask about:
Dysuria
Frequency
Urgency
Haematuria
Flank pain
Renal colic can present dramatically, while urinary tract infections may produce surprisingly vague abdominal discomfort, particularly in older adults.
Gynaecological History
For any patient of childbearing age, pregnancy should remain part of your differential diagnosis unless confidently excluded.
Sensitive communication is essential.
Questions may include:
When was your last menstrual period?
Is there any possibility you could be pregnant?
Any abnormal vaginal bleeding?
Any vaginal discharge?
These questions can feel uncomfortable for students.
They become significantly easier with practice.
Remember:
📌 You are not asking because you are curious. You are asking because pregnancy changes your differential diagnosis completely.
Conditions such as ectopic pregnancy are time-critical and potentially life-threatening.
Testicular Pain
Male patients may present with abdominal pain when the pathology lies elsewhere.
Always consider whether pain could originate from the testes.
Testicular torsion is a surgical emergency.
Never ignore lower abdominal pain associated with acute scrotal symptoms.
Past Medical History
Students often ask:
"Do you have any medical problems?"
Then move on.
Instead, interpret every condition.
Examples include:
Previous abdominal surgery?
→ Adhesions increase bowel obstruction risk.
Gallstones?
→ Biliary pathology becomes more likely.
Atrial fibrillation?
→ Mesenteric ischaemia should enter your differential.
Inflammatory bowel disease?
→ Flare-up or obstruction becomes possible.
Every condition should alter your thinking.
Medication History
Medication history should answer:
"Could this explain the presentation?"
Examples:
NSAIDs
→ Increased peptic ulcer risk.
Anticoagulants
→ Increased bleeding risk.
Steroids
→ Immunosuppression and atypical presentations.
Diabetic medication
→ Consider diabetic ketoacidosis or hypoglycaemia.
Previous Surgery
Previous surgery is often more important than students realise.
Abdominal surgery significantly increases the likelihood of adhesive bowel obstruction.
Never skip this question.
Common Student Mistake
Many students collect huge amounts of information but never use it.
Good clinicians don't simply gather facts.
They constantly ask:
What does this make more likely?
What does this make less likely?
Does this increase or decrease my concern?
History taking is not a memory exercise.
It is a process of building and continually refining a working clinical picture.
PocketClinician Tip
One of the biggest challenges during abdominal assessments is remembering all the relevant questions without missing important red flags.
The PocketClinician Student Paramedic Pocketbook includes a dedicated abdominal assessment section with structured history-taking prompts, review of systems questions, key positive and negative findings, and documentation guidance. Rather than relying on memory alone, it provides a logical framework that helps you focus on the patient while ensuring your assessment remains thorough and clinically relevant.
Part 3 - Physical Examination: Turning Information into Clinical Judgement
By the time you begin examining the abdomen, you should already have a working clinical impression.
You should know:
Where the pain is
How it started
What symptoms accompany it
Which serious conditions you're considering
The purpose of the examination is not to "find the diagnosis".
Its purpose is to:
Confirm or challenge your differential diagnoses
Identify signs of serious pathology
Determine whether the patient appears to be deteriorating
Support safe clinical decision-making
Your examination should always be systematic. Randomly pressing different areas of the abdomen is uncomfortable for the patient and rarely produces useful clinical information.
Inspection
Before touching the patient, stop and observe.
Inspection begins the moment you see the patient—not the moment you expose the abdomen.
Ask yourself:
Does the patient look unwell?
Are they pale?
Are they clammy?
Are they guarding the abdomen?
Are they lying completely still?
Are they restless?
Do they appear distressed?
Often, these observations provide more diagnostic value than palpation.
Observe how the patient moves
Movement can tell you a remarkable amount.
Patients with peritonitis often avoid movement because every small motion worsens their pain.
By contrast, patients with renal colic frequently cannot stay still. They may pace around the room, constantly changing position in an attempt to become comfortable.
Neither behaviour is diagnostic on its own.
However, both should influence your clinical reasoning.
Look for abdominal distension
Abdominal distension may suggest:
Bowel obstruction
Ascites
Severe constipation
Massive organ enlargement
Pregnancy
Ask yourself:
Is this abdomen larger than expected?
Is the distension symmetrical?
Does it fit with the history?
Distension combined with severe pain, vomiting and inability to pass stool or flatus should immediately increase your suspicion of bowel obstruction.
Surgical scars
Never ignore previous surgical scars.
They provide important clues about previous operations.
Examples include:
Midline laparotomy
Appendicectomy
Caesarean section
Laparoscopic procedures
Why does this matter?
Previous abdominal surgery significantly increases the risk of adhesive bowel obstruction, one of the common causes of acute abdominal pain.
Skin changes
Although uncommon, certain skin findings should never be ignored.
Cullen's sign
Periumbilical bruising.
May indicate intra-abdominal bleeding or severe pancreatitis.
Usually represents relatively late disease.
Grey Turner's sign
Bruising over the flanks.
May indicate retroperitoneal haemorrhage, including severe pancreatitis.
Again, this is an uncommon but significant finding.
Clinical Pearl
Do not spend your placement hoping to find Cullen's or Grey Turner's signs.
Many experienced paramedics never see them.
Know what they mean, but never rely on them to diagnose serious illness.
Palpation
Palpation is often where students become nervous.
Remember:
The goal is not to make the patient hurt.
The goal is to gather useful clinical information while causing as little discomfort as possible.
Always explain what you're about to do.
Warm hands where possible.
Watch the patient's face, not just your own hands.
Often, facial expression tells you more than verbal responses.
Start away from the pain
This is one of the oldest principles of abdominal examination, and for good reason.
Begin palpation in the area least likely to be painful.
This allows the patient to relax and helps you appreciate what "normal" feels like before approaching the affected region.
Jumping straight onto the painful area often causes voluntary guarding and limits the usefulness of the examination.
Light palpation
Initially assess for:
General tenderness
Localised tenderness
Guarding
Obvious masses
Observe both:
What the patient says
What their body does
Some patients instinctively tense their abdominal muscles before you've even touched them because they anticipate pain.
Good communication often reduces this considerably.
Deep palpation
If appropriate and tolerated, deeper palpation may help identify:
More localised tenderness
Abdominal masses
Organ enlargement
Never force an examination.
If the patient is clearly distressed or guarding significantly, further palpation is unlikely to provide useful additional information.
Guarding versus rigidity
These terms are often used interchangeably—but they are different.
Guarding
Guarding is contraction of the abdominal muscles in response to pain.
It may be:
Voluntary
Involuntary
Patients often relax when reassured or distracted if guarding is voluntary.
Rigidity
Rigidity is involuntary muscle contraction caused by peritoneal irritation.
Unlike voluntary guarding, rigidity generally persists despite reassurance.
It should immediately increase concern for significant intra-abdominal pathology.
📌 Rigidity is uncommon. But when present, it is an important clinical finding.
Rebound tenderness
Students are often taught to actively test for rebound tenderness.
In modern practice, this should be approached cautiously.
Rapidly removing your hand to provoke pain can cause unnecessary discomfort and rarely changes immediate pre-hospital management.
Instead, if you suspect peritonism, rely on the wider clinical picture:
Pain worsened by movement
Guarding
Rigidity
Significant tenderness
General appearance
These findings usually provide sufficient evidence to justify urgent hospital assessment.
Think Like a Paramedic
Ask yourself:
"Will performing this examination change my management?"
If the answer is no, reconsider whether it is necessary.
Patients should never undergo painful examination simply because it appears in a textbook.
Percussion
Percussion receives far more emphasis in traditional medical examinations than it usually does in routine ambulance practice.
Nevertheless, understanding its purpose is useful.
Percussion may help identify:
Generalised tenderness
Tympanic bowel distension
Ascites
However, remember:
Your clinical decision-making should rarely depend on percussion findings alone.
History, inspection, palpation and physiological assessment remain significantly more valuable.
Auscultation
Many students expect bowel sounds to play a major role in abdominal assessment.
In reality, bowel sounds have limited value in the pre-hospital setting.
Why?
Because:
Normal bowel sounds do not exclude significant pathology.
Reduced bowel sounds are non-specific.
Absent bowel sounds can be difficult to confirm reliably, particularly in noisy environments.
Auscultation may be appropriate in some settings, but it should never delay assessment, treatment or transport.
Special tests
Several named examination signs are commonly taught during university training.
Understanding them is useful.
Attempting to forcefully elicit them in every patient is not.
Murphy's sign
Murphy's sign assesses for inflammation of the gallbladder.
During gentle palpation of the right upper quadrant, the patient is asked to take a deep breath.
A sudden arrest of inspiration due to pain may suggest acute cholecystitis.
Remember:
Murphy's sign is only one finding.
Interpret it alongside:
Fever
Right upper quadrant tenderness
Nausea
Clinical history
McBurney's point tenderness
Tenderness over McBurney's point may support appendicitis.
However:
Early appendicitis frequently presents with vague central abdominal pain before localising.
A normal examination early in the illness does not exclude appendicitis.
Rovsing's sign
Pain felt in the right iliac fossa during palpation of the left iliac fossa has traditionally been associated with appendicitis.
Again:
This is a supporting sign, not a diagnostic test.
Do not overemphasise isolated examination findings.
Examination is only one part of assessment
One of the biggest mistakes students make is placing excessive weight on physical examination.
Remember:
Patients with serious pathology can have surprisingly subtle abdominal findings.
Conversely, patients with severe tenderness may have relatively benign conditions.
Your examination should always be interpreted alongside:
History
Observations
General appearance
Risk factors
Response over time
Common Student Mistake
Many students believe:
"If I can't feel anything abnormal, the abdomen must be normal."
This is incorrect.
Abdominal examination has limitations.
Some dangerous conditions, including mesenteric ischaemia, early appendicitis and abdominal aortic aneurysm may initially produce relatively unremarkable examination findings.
Never allow a reassuring abdominal examination to override a concerning history or an unwell patient.
PocketClinician Tip
The PocketClinician Student Paramedic Pocketbook includes a dedicated abdominal assessment section with illustrations, key examination findings, positive and negative signs to document, and clinically relevant special tests. Rather than trying to remember every examination manoeuvre under pressure, it provides a structured framework that helps you examine the abdomen systematically and document your findings confidently during placement and OSCEs.
Part 4 - Clinical Reasoning: Turning Findings into Decisions
By this point you have:
Taken a structured history
Performed a systematic examination
Recorded observations
Developed a working impression
Now comes the difficult part.
What does it all mean?
One of the biggest misconceptions among student paramedics is believing that assessment should always end with a diagnosis.
In reality, your assessment should end with a safe, defensible clinical decision.
Pre-hospital clinicians work with incomplete information.
You won't have:
Blood results
CT imaging
Ultrasound
Surgical opinion
Therefore your role is rarely to diagnose appendicitis, pancreatitis or bowel obstruction with certainty.
Your role is to decide:
How concerned should I be?
Does this patient require immediate hospital assessment?
Could this deteriorate rapidly?
What is the safest course of action?
That is the essence of paramedic clinical reasoning.
The Life-Threatening Conditions You Must Never Miss
When assessing abdominal pain, always begin with the conditions that could seriously harm or kill the patient if missed.
Not because they're the most common.
Because they're the most dangerous.
Abdominal Aortic Aneurysm (AAA)
Although uncommon, a ruptured AAA is one of the most time-critical abdominal emergencies encountered in pre-hospital care.
Risk factors include:
Increasing age
Male sex
Smoking history
Hypertension
Known aneurysm
Presentation may include:
Sudden abdominal pain
Back pain
Collapse or syncope
Hypotension
A pulsatile abdominal mass (although this is often absent)
Remember:
Not every patient presents with the classic triad.
A patient with sudden back pain who becomes hypotensive deserves immediate concern.
Ectopic Pregnancy
Every clinician should ask themselves one question when assessing any patient of childbearing age:
Could this be pregnancy related?
Ectopic pregnancy remains a life-threatening emergency.
Red flags include:
Lower abdominal pain
Vaginal bleeding
Shoulder tip pain
Collapse
Syncope
Never allow embarrassment to prevent appropriate questioning.
Patients expect healthcare professionals to ask clinically relevant questions.
Mesenteric Ischaemia
Students rarely consider mesenteric ischaemia because it receives relatively little teaching.
However, one phrase should stay with you:
Pain out of proportion to examination.
A patient with severe pain but relatively minimal abdominal tenderness should make you pause.
Risk factors include:
Atrial fibrillation
Peripheral vascular disease
Increasing age
Although uncommon, delayed recognition carries an extremely high mortality.
Bowel Obstruction
Think bowel obstruction when patients present with:
Vomiting
Abdominal distension
Constipation
Failure to pass flatus
Colicky pain
Previous abdominal surgery significantly increases risk due to adhesions.
Perforated Viscus
Perforation should be considered in patients with:
Sudden severe abdominal pain
Generalised tenderness
Guarding
Rigidity
Signs of sepsis or shock
These patients often deteriorate rapidly.
Sepsis
Abdominal infections remain an important cause of sepsis.
Students should continually ask:
Could infection explain this presentation?
Is this patient becoming septic?
Watch for:
Fever or hypothermia
Tachycardia
Tachypnoea
Hypotension
Altered mental state
Remember:
Normal observations early in sepsis do not exclude serious illness.
Think Like a Paramedic
A useful mental question is:
"What could kill this patient before they reach hospital?"
Once you've considered those conditions, you can begin thinking about the more common, less immediately dangerous causes.
This simple habit dramatically improves clinical prioritisation.
Red Flags That Should Change Your Management
Certain findings should immediately lower your threshold for urgent transport and escalation.
These include:
Haemodynamic instability
Syncope or near-syncope
Persistent hypotension
Severe, worsening pain
Peritonism
Gastrointestinal bleeding
Haematemesis
Melena
Significant abdominal distension
Pregnancy with abdominal pain
Immunosuppression
Significant pain in older adults without obvious cause
None of these findings provide a diagnosis.
All of them increase risk.
The Importance of Reassessment
Abdominal pain is dynamic.
Patients who appear stable initially may deteriorate during transport or while awaiting assessment.
Reassess:
Pain severity
Heart rate
Blood pressure
Respiratory rate
Mental state
Overall appearance
One set of observations provides a snapshot.
Repeated assessment provides a trend.
Trends are often far more valuable.
Common Student Mistakes
Over years of teaching and supervising students, several patterns appear repeatedly.
Focusing on diagnosis too early
Students often become determined to identify exactly what condition the patient has.
Instead, focus on:
Identifying risk
Recognising deterioration
Making safe decisions
Diagnosis will often come later.
Ignoring atypical presentations
Not every patient reads the textbook.
Older adults, diabetic patients and immunocompromised patients frequently present differently from younger, healthier individuals.
Remain curious.
Remain cautious.
Being falsely reassured by normal observations
Normal observations should never override:
An unwell appearance
Significant pain
Red flags
Concerning history
Always treat the whole patient.
Not documenting clinical reasoning
Good documentation doesn't simply describe what happened.
It explains:
What you considered
What concerned you
Why you made your decision
If challenged later, your documentation should allow another clinician to follow your thinking.
OSCE Tip
Students often assume they lose marks because they forgot one question.
More commonly they lose marks because they fail to explain their reasoning.
Don't simply say:
"The patient has abdominal pain."
Instead say:
"The patient has worsening right iliac fossa pain associated with anorexia and localised tenderness. Although appendicitis cannot be confirmed pre-hospitally, the presentation raises concern for acute intra-abdominal pathology requiring hospital assessment."
That demonstrates clinical reasoning.
Examiners reward thought processes, not just checklists.
Putting Everything Together
A good abdominal assessment should naturally flow like this:
Initial impression
↓
Primary survey
↓
Pain assessment
↓
Associated symptoms
↓
Past medical, medication and surgical history
↓
Targeted abdominal examination
↓
Interpret findings
↓
Identify red flags
↓
Consider life-threatening pathology
↓
Reassess
↓
Communicate and document your reasoning
Notice something important?
The diagnosis isn't the final step.
The decision is.
Final Clinical Perspective
Abdominal pain remains one of the most challenging presentations in pre-hospital care because uncertainty is unavoidable.
You will not diagnose every patient correctly.
Neither will experienced clinicians.
What defines safe paramedic practice is not diagnostic perfection.
It is the ability to:
Recognise serious illness
Identify deterioration
Appreciate uncertainty
Make safe, defensible decisions
Escalate when appropriate
As a student paramedic, that is exactly what you should be striving for.
Supporting Your Learning on Placement
Developing confidence in abdominal assessment takes time, repetition and exposure to real patients. However, having a structured approach significantly reduces cognitive overload and makes it easier to think clearly under pressure.
The PocketClinician Student Paramedic Pocketbook was created specifically for those moments when you know whatyou should be doing but struggle to remember every question, examination finding or red flag.
Inside the abdominal assessment section you'll find:
A structured assessment framework that follows the approach outlined in this guide
History-taking prompts, including gastrointestinal, urinary and gynaecological questions
Positive and negative examination findings to document
Important special tests and what they suggest
Red flags that should increase concern for serious pathology
Documentation prompts to support clear, defensible patient records
Practical placement tips designed specifically for UK student paramedics
Rather than replacing your clinical reasoning, the Pocketbook is designed to support it, giving you a logical framework so you can spend less time worrying about what to ask next and more time focusing on your patient.
Whether you're preparing for your first placement, revising for university, or getting ready for an OSCE, it has been designed to fit in your pocket and become a resource you'll refer back to throughout your training.
Key Learning Points
Before finishing this guide, remember these principles:
Abdominal pain is a symptom, not a diagnosis.
Always perform a primary survey before focusing on the abdomen.
Use your history to narrow differential diagnoses, not simply complete a checklist.
Observe the patient before you examine them.
A normal abdominal examination does not exclude serious pathology.
Always consider life-threatening causes first.
Reassessment is essential.
Clinical reasoning is more important than diagnostic certainty.
Your final responsibility is to make a safe, defensible clinical decision.
Frequently Asked Questions
What is the most important part of an abdominal assessment?
There isn't one single most important part. A safe abdominal assessment combines a structured history, careful examination, interpretation of observations and ongoing clinical reasoning. Often, the patient's history provides more diagnostic value than the physical examination alone.
Should paramedics perform rebound tenderness?
Routine forceful testing for rebound tenderness is generally unnecessary in pre-hospital care. If peritonism is suspected, the wider clinical picture—including guarding, rigidity, pain on movement and the patient's overall condition—is usually sufficient to guide management.
Can a patient have serious abdominal pathology with normal observations?
Yes. Conditions such as early appendicitis, mesenteric ischaemia and abdominal aortic aneurysm may initially present with relatively normal observations. Observations should always be interpreted alongside the patient's history, examination findings and overall appearance.
How can I improve my abdominal assessment on placement?
The best way to improve is through repeated practice using a consistent framework. Reflect on each patient you assess, review your documentation afterwards, ask your mentor for feedback, and use structured resources such as the PocketClinician Student Paramedic Pocketbook to reinforce your assessment approach between shifts.